


Carbohydrate counting
Carbohydrate counting is often used by people using bolus insulin (usually for type 1 diabetes) to more accurately estimate their meal time insulin doses. It is useful for people with type 2 diabetes to have an awareness of the carbohydrate amount in food, particularly if they are on regular insulin injections.
The impact of carbohydrate on blood glucose
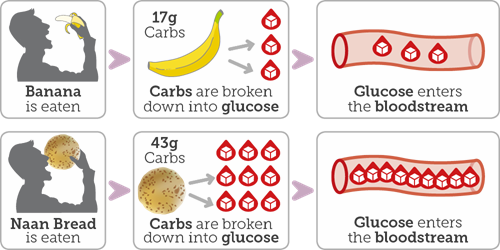
Carbohydrate is a nutrient that is an important source of energy.
All carbohydrates when digested are broken down into glucose which then enters into the bloodstream. When insulin is available the glucose is carried into the body’s cells to provide energy.
The rise in blood glucose from carbohydrates will depend on the following factors:
- The amount and type of carbohydrate eaten.
- Activity and exercise undertaken.
- If using insulin, then the amount of insulin circulating in your blood stream. Factors affecting this including the insulin type, dose and time taken, but also factors such as which part of the body you've injected, length of needle (short needles 5mm or less are best) and whether you have any skin changes in your injection sites (lipohypertrophy or "lumpy" skin)
The role of carbohydrate counting in management of blood glucose
To achieve ideal blood glucose control, the amount of carbohydrate eaten needs to be balanced with the amount of bolus insulin taken. There are two ways to approach this:
- Eating similar amounts of carbohydrates at the same time each day.
- Learning to adjust your bolus insulin dose to match the amount of carbohydrate eaten.
Understanding and implementing the principles of carbohydrate counting will assist in keeping blood glucose levels as near to normal as possible.
Twice daily mixed insulin regimen
Insulin used twice daily may contain a mixture of shorter and intermediate acting insulin e.g. Humulin M3; Novomix 30 and is taken twice a day at breakfast and evening meal. Individuals who are on this regimen, are unable to adjust their insulin, but carbohydrate counting can be applied to maintain similar amounts at meals.
Multiple daily injection insulin regimen / basal bolus therapy
This regime includes an injection of bolus insulin e.g. Humalog or Novorapid at each meal. Those who are on this regimen are able to adjust their bolus insulin at each meal time. The amount of bolus insulin taken is directly related to the amount of carbohydrate consumed.
Carbohydrate counting
The first step in the process is to identify all items that contain carbohydrate.
There are various resources which can help, these include:
- Carbohydrate reference lists / counting tables.
- Food labels and diaries.
- Handy household measures e.g. scales, cups, spoons.
- Apps e.g. Carbs and Cals app.
- Reference books e.g. Carbs and Cals; Cook and Count.
- Restaurant websites.
Next, it is necessary to work out the carbohydrate content of all foods and drinks consumed.
Carbohydrates can be counted in two ways; in grams or as carbohydrate portions. One carbohydrate portion (CP) is equal to 10 grams of carbohydrate. Your diabetes care team will guide you on which approach is used at your centre.
Example: Using Carbohydrate Reference List (grams)
|
Lunch |
Carbohydrate Content |
|
2 Slices Thick White Toast |
44 grams |
|
Cheese and Cold Ham |
0 grams |
|
Packet Crisps |
17 grams |
|
Yoghurt |
19 grams |

The total carbohydrate content of the above lunch is 80 grams.
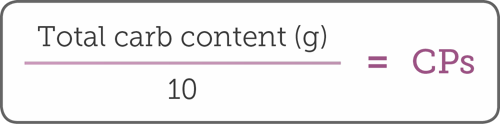
As every 1 CP contains 10 grams of carbohydrate, calculating the total amount of carbohydrate in grams allows for the CP content of the meal to also be established:
CP Content = Total Amount of Carbohydrate in Meal in grams divided by 10
CP Content = Total Amount of Carbohydrate in Lunch 80 grams divided by 10
The above lunch of 80 grams of carbohydrate is equivalent to 8CPs.

Calculating bolus dose
To work out the bolus dose, you will need:
1. Personal Insulin to Carbohydrate Ratio (ICR).
- This is the amount of bolus insulin you need to inject at meals for a certain amount of carbohydrate.
- The ICR will vary from person to person and can be different for each meal.
- A starting ICR for most individuals is 1 unit of bolus insulin for every 10g of carbohydrate (1 CP). This is based upon the fact that 10 grams of carbohydrate (1 CP) will increase blood glucose by 2 – 3 mmols and 1 unit of bolus insulin will reduce blood glucose by the same amount.
- To work out the most suitable starting ICR for you, it is important to talk to a member of your diabetes care team.
2. The total amount of carbohydrate consumed (grams / CPs).
3. When you know your ICR and have worked out the carbohydrate content of your meal, as the example below illustrates, you can calculate the amount of bolus insulin you need.
Example: calculating the bolus dose
For the above lunch of 80 grams of carbohydrate / 8 CPs, with an ICR of 1 unit for every 10 grams / 1 CP, the required bolus dose is 8 units.
Insulin bolus dose adjustment and carbohydrate counting
When you feel confident in this approach you should be able to:
- Vary the times you eat and the amount of carbohydrate you eat.
- Predict blood glucose response from different foods.
Additional resources
As you must be able to accurately calculate the amount of carbohydrate you eat and drink before adjusting your bolus dose, a carbohydrate log can help you demonstrate this.
It can also be useful to record a detailed diary which outlines carbohydrate eaten, blood glucose, activity, bolus and basal insulin.
An online resource which will provide additional information on the key principles of carbohydrate counting and insulin dose adjustment BERTIE has been developed by the Bournemouth Diabetes Team.
Carbohydrate counting and insulin dose adjustment is a complex process. Before implementing this strategy, it is important to have the support and guidance of your diabetes care team.
Resources
Carbs and cals book
This visual book contains 1,700 food photos, showing the fibre content for each portion to help you achieve your 30g fibre each day, as well as carbs, calories and other nutrients
Carbs and cals app
This visual app is perfect for those counting calories, monitoring carbs, boosting fibre, looking to improve portion control or lose weight.
World foods book
If you’re from an African, Arabic, Caribbean or South Asian background, this book helps you understand the carbs in the food you eat. Its visual style makes it easy to select portion sizes.